Cervical / Lumbar Disc Surgery
Cervical Disc Surgery
Prolapsed cervical intervertebral disc when causes significant compression on the spinal cord or nerve root, requires surgery. It usually occurs as a result of sudden jerk to neck, weight lifting, degenerative causes or as a result of trauma.
Patient may complaint of neck pain, which may radiate down to one or both upper limbs, along with weakness and/or tingling numbness in upper or lower limbs. Patient may complain of imbalance in walking with/without bladder bowel involvement. Diagnosis is by MRI of the cervical spine. CT scan of the spine may be needed at times for additional information on the bony architecture. Surgery for the cervical disc can be done from the anterior approach, front of the neck and less often via the posterior region. Previously surgery involved only discectomy, ie removing of the disc. However, recently along with discectomy, fusion and fixation of the spine is done with a bone graft and metallic implants, cervical plate and screws.
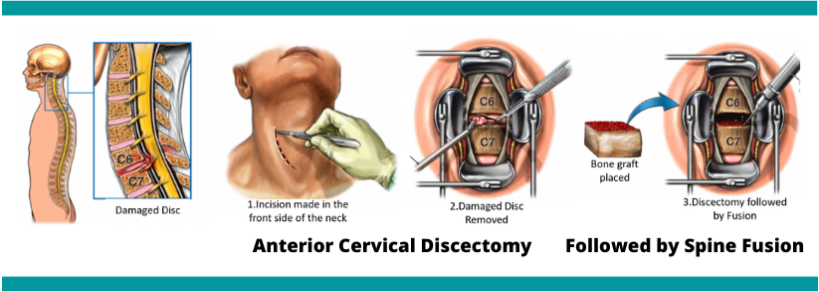
Surgery is done under general anasthesia. It involves placing a cut on the front of the neck, usually along the skin crease. The level is localised using C arm. Muscle dissection is done and the spine is reached. Operating microscope is then brought in the field and discectomy is done under vision from the microscope. Complete disc removal is done followed by cutting the PLL (posterior longitudinal ligament) so as to free the spinal cord. Bone graft is harvested from the iliac crest which involves a separate incision on the iliac region. Appropriate size graft is placed in the disc space and a cervical plate is put over it and fixed with screws in the adjoining vertebral bodies. Alernatively, cage with plate is available with prefixed space for bone graft and predirected screw slots.
In certain traumatic cases or degenerative cases, the vertebral body may be removed to free the spinal cord – corpectomy and the defect is filled with bone graft and overlaid by a cervical plate or an expandable mesh cage filled with bone graft is used.
Less often cervical discectomy may be done from the back of the neck – posterior approach. It may be done for large soft discs that are lateral to the spinal cord. It involves a small incision at the back of the neck and removal of the small portion of the bone and approaching the disc via microscope. Extruded fragment of the disc is removed and nerve root freed from the pressure. Fixation is not needed is the main advantage of this procedure. However, entire portion of disc is not removed and patient may require anterior surgery at later date.
A cervical collar is advised after surgery on the cervical spine. Mobilisation is done by the physiotherapy and rehabilitation team.
Lumbar Disc Surgery
Lumbar disc herniations occur as a result of heavy weight lifting , sudden jerk to the lower back, long time overuse of the back or as a result of trauma.
Patient experiences back pain that may radiate down one or both legs, in addition to feeling of tingling numbness in the legs with or without weakness of the legs. Some patients may complain of bladder bowel involvement symptoms. Patient may feel back pain on prolonged standing or walking.
MRI clinches the diagnosis and patient with significant disc herniation compressing the thecal sac or nerve root are advised surgery.
Surgery for herniated lumbar disc is done via an incision on the lower back. General anaesthesia is administered. Patient is turned prone on bolsters or spine frame. Conventional or open technique involved placing an incision on the lower back, dissecting the muscles and exposing the lamina. Laminectomy is done with Kerrison punches and ligamentum flavum is excised, discectomy is done and the thecal sac is freed.
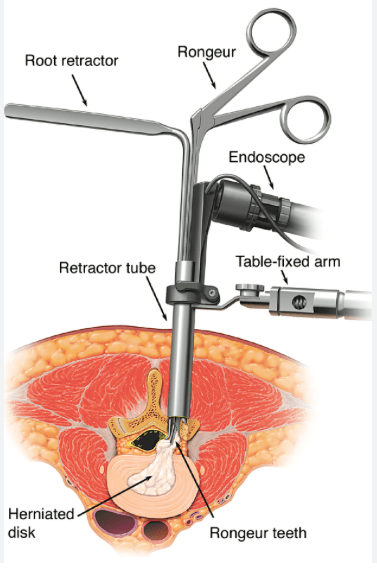
Technical advancement involves using the microscope or the endoscope for removing the extruded disc. Sequential tubular retractors are inserted via a small skin incision and muscles are split and the tube is docked under C arm guidance. Using a microscope or endoscope, part of the lamina is removed and ligamentum flavum is excised and the extruded disc is removed. Advantages of minimally invasive approach includes smaller incision, less muscle dissection and less pain, lesser blood loss, faster recovery and earlier return to work.
Looking for Neuro
Surgeon?
Simply give us a call and book an appointment for yourself. We are here to help. Walk into our Hospital and let us take a closer look to suggest the best treatment you need.